
日本語訳監修: 木下佳代子 ジェックス参与
今月は、緩和ケア患者さんのケアのゴールについて、あなたとあなたのチームがどのように理解しているのかについて、改めて考えてみたいと思います。
私たちは、患者さんが亡くなる前に、何日も何週間も「無益な」治療を受けているのを見たことがあります。 なぜこのようなことが起こったのか、不思議に思いませんか?
以前、緩和ケアの言葉や正しい意味の使い方が重要であることをお話ししました。 緩和ケアの定義は、時に難しい言葉であります。
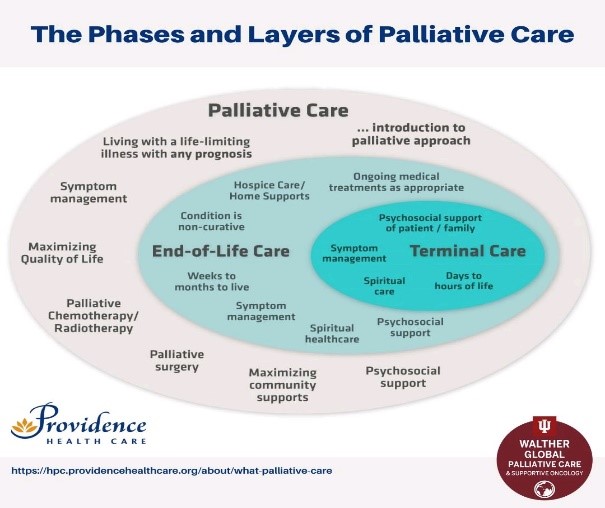
最近見つけたこの図は、緩和ケアの段階と層を明確に定義し、緩和的アプローチ、終末期ケア、ターミナルケアという言葉の明確な違いを表現しています。
-
おそらく、唯一欠けているのは死別の段階かもしれません。 しかし、この図は、患者や家族とのケアの目標の設定や、患者が新しい段階に移る際の再確認など、どのような会話をすべきかを考え始めるための枠組みを提供してくれます。 このような枠組みは、緩和ケアの患者さんやご家族、医療チーム内でどのようなコミュニケーションをとるべきかを考えるのに役立つのではないでしょうか? この点に関する皆さんのご意見をお聞かせください。
- ● 例えば、引継ぎのときに、もし患者が終末期の患者であれば緩和の患者と呼ばない、逆に余命数週間から数日の終末期の患者でない場合、
その患者を終末の患者と呼ばない。 - ● がんや心不全などの慢性疾患に対して緩和的なアプローチをとる場合、患者さんの死ぬ前にやっておきたいことを書き出したリスト(バケ
ットリスト)についての会話を求めること。 - ● 提供されているケアや医療チームと患者・家族との会話が、患者の置かれている段階と一致しない場合、患者の医療チームのメンバーにつ
いて専門的に話しあったり、質問したりすることができること。
これまで述べてきたように、医療チームが緩和ケア用語を正しく使うことは、患者さんやその家族、そしてより広いコミュニティが、緩和ケアとは何かを正確に理解することにもつながるのです。 そうすることで、患者さんのQOLの意味やそれを支えるプランを見つけ出すことについて、より早い段階での紹介や話し合いが促されることが期待されます。 また、患者さんが他の段階を経ていく中で、特定の段階で何を期待するかについて、ご家族と有意義な会話ができるようになります.
- ● 例えば、引継ぎのときに、もし患者が終末期の患者であれば緩和の患者と呼ばない、逆に余命数週間から数日の終末期の患者でない場合、
-
この図は、緩和ケアの組織方針の中でも使用することができ、チーム全員が同じ用語を使用し、患者や家族のニーズについて言語と理解を共有するという事をサポートすることができるでしょう。
また、下記に示した WHO Palliative Care key facts も参考になるかと思います:
https://www.who.int/news-room/fact-sheets/detail/palliative-care
-
もし、追加情報が必要な分野があれば、julie@palliativeeducation.com までリクエスト(英語または日本語)を転送していただければ、確実に議論させていただきます。
あなたのご様子もお聞かせください。 緩和ケアに関する皆さんの考えや経験を共有し、お互いに学び続けられるよう、楽しみたいと思います。
来月のキャッチアップを楽しみにしています。
お元気で、 ジュリー
[事務局より]
ジュリーさんは、皆様からの感想、質問などをお待ちしています。
-
Disclaimer: June 2022 免責条項:
Australian International Palliative Education and Consultancy Services (AIPEACS) は、Julie’s Corner シリーズ内の内容につき正確な情報の提供に細心の注意を注いでいますが、特にある事柄についての専門的意見を提供するものではありません。このシリーズに含まれる情報は、独立した専門家の見解に取って代るものではありません。また、医療上の助言として利用したり、何らかの疾患の治療、手当、又は、予防のために使用されるものではありません。
AIPEACSは、このシリーズにより提供される情報の利用、依存によるいかなる法的責任、怪我、紛失、損害については、責任は負いません 。
Australian International Palliative Education and Consultancy Services Pty. Ltd -
Julie’s Update: June 2022 (原文)
-
This month I would like us to again think about how you and your team communicate their understanding of the goals of care for a palliative care patient.
We have all seen patients have “futile” treatment for days or weeks before they die. Do you wonder why this has occurred?
We have discussed previously the importance of words and assigning the correct meaning of palliative care. I know for some, defining palliative care is sometimes a difficult term to describe.
I came across this diagram recently that clearly defines the phases and layers of palliative care, articulating the distinct differences between the words palliative approach, end of life care and terminal care.
-
Perhaps the only phase that may be missing is bereavement. Never the less, the diagram provides us with a framework to start thinking about the types of conversations, including the establishment of goals of care with patients and families and revisiting these, as patients move to a new phase. I wonder would this type of framework assist the types of communications we should be having with palliative care patients and families and within the health team? I would be very interested in your thoughts on this.
For example:
- Not calling a patient palliative in handover if they are in the terminal phase, and vice versa not calling a patient terminal when they are not in the last few weeks or days of life.
- Seeking conversations with patients about their “bucket list” when they are adopting a palliative approach to their disease, whether that be cancer or chronic diseases such as heart failure.
- Being able to professionally discuss or question members of the patient’s health care team, when the care being provided and conversations with the health care team and the patient and family do not match the phase they are in.
As we have discussed previously, ensuring the health team use palliative care terminology correctly will also support the patient, their families and the wider community, in their understanding of exactly what palliative care is. This will hopefully encourage earlier referral and discussions about the meaning of quality of life for patients and development of plans to support this. Also to have meaningful conversations with families as to what to expect in particular phases as well, as patients progress through the other phases.
The diagram could also be used within a palliative care organisational policy, which would ensure all of the team are using the same terminology and would support a shared language and understanding of the needs of the patient and families.
-
Another link you may find helpful to refresh is the WHO Palliative Care key facts
-
https://www.who.int/news-room/fact-sheets/detail/palliative-care
-
If you have any particular areas you would like additional information on, please forward your request (either in English or Japanese) to julie@palliativeeducation.com and I will ensure this is discussed.
Please let me know how you are going. I will enjoy sharing your thoughts and experiences on palliative care, so that we can continue to learn from each other.
I am looking forward to our next month’s catch up.
-
-
Take care, Julie
-
-